CHIP's Milestones and the Transformation of Children's Health Coverage

CHIP has helped millions of children get health insurance.
- The number of uninsured children dropped to 3.9 million in 2022, with many states seeing big improvements.
- Since 1998, CHIP enrollment has grown from 665,000 to 8.1 million children.
Children with coverage see better health, more doctor visits, and fewer unmet needs.
Key Takeaways
- CHIP has helped millions of children get health insurance, cutting the uninsured rate in half since 1997 and expanding coverage to more families.
- States use CHIP’s flexibility to cover more children, offer important benefits like dental and mental health care, and make enrollment easier for families.
- Children with CHIP coverage get better health care, including checkups and vaccines, which leads to healthier lives and stronger futures.
CHIP Milestones and Achievements

Launch and Early Impact
The Children’s Health Insurance Program (CHIP) began in 1997 as part of the Balanced Budget Act. This law created a new way for states to help children from families who could not afford private insurance but earned too much for Medicaid. Over time, Congress reauthorized CHIP, most notably with the Children’s Health Insurance Program Reauthorization Act of 2009 (CHIPRA). This act extended funding and made it easier for families to enroll their children. CHIPRA also set up the Medicaid and CHIP Payment and Access Commission (MACPAC) to watch over how the program worked.
Key legislative milestones that shaped CHIP:
- Creation under the Balanced Budget Act of 1997.
- CHIPRA of 2009 extended funding and improved enrollment.
- MACPAC established for oversight and policy guidance.
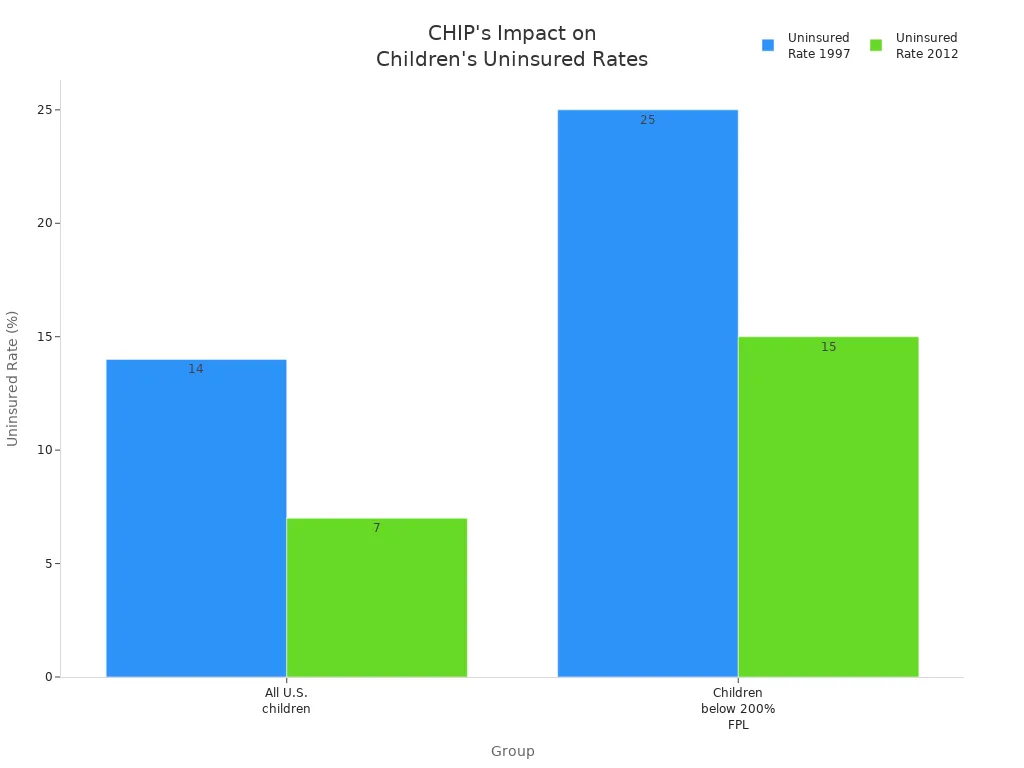
CHIP’s early years saw big changes in health coverage for children. The uninsured rate for all U.S. children dropped from 14% in 1997 to 7% by 2012. For children in families below 200% of the federal poverty level, the uninsured rate fell from 25% to 15%. Hispanic children, who started with higher uninsured rates, saw even sharper declines.
| Group | Uninsured Rate Before CHIP (1997) | Uninsured Rate After CHIP (2012) | Change Observed |
|---|---|---|---|
| All U.S. children | 14% | 7% | Reduced by half |
| Children below 200% FPL (target) | 25% | 15% | Significant decline |
| Hispanic children | Higher initially | Sharper decline | Noted improvement |
CHIP and Medicaid together expanded coverage to 37% of all children in the country. Even during tough economic times, CHIP acted as a safety net. When employer-based insurance dropped, CHIP kept children covered.
Expanding Eligibility and Coverage
CHIP started by covering children in families with incomes up to 200% of the federal poverty level. Over time, many states raised these limits. Some states now cover children up to 400% of the federal poverty level. States also have the option to cover pregnant women and lawfully present immigrants without a waiting period. For example, California covers children up to 317% of the federal poverty level, and Minnesota covers children up to age 2 with incomes up to 283% of the federal poverty level.
States use different rules for who can get CHIP. These rules include income, age, residency, and citizenship or immigration status. States can also choose to offer 12-month continuous eligibility, which helps children stay insured even if their family’s income changes during the year. States with this policy saw smaller drops in coverage during recent changes to Medicaid rules.
Notable achievements of CHIP in expanding access:
- Filled the gap for children in families earning too much for Medicaid but too little for private insurance.
- Helped reduce the uninsured rate among children from 14% to 7% by 2012.
- Provided a safety net during economic downturns.
- Covered important benefits like dental, vision, and therapies often missing from private plans.
- Improved access to doctors, specialists, and preventive care.
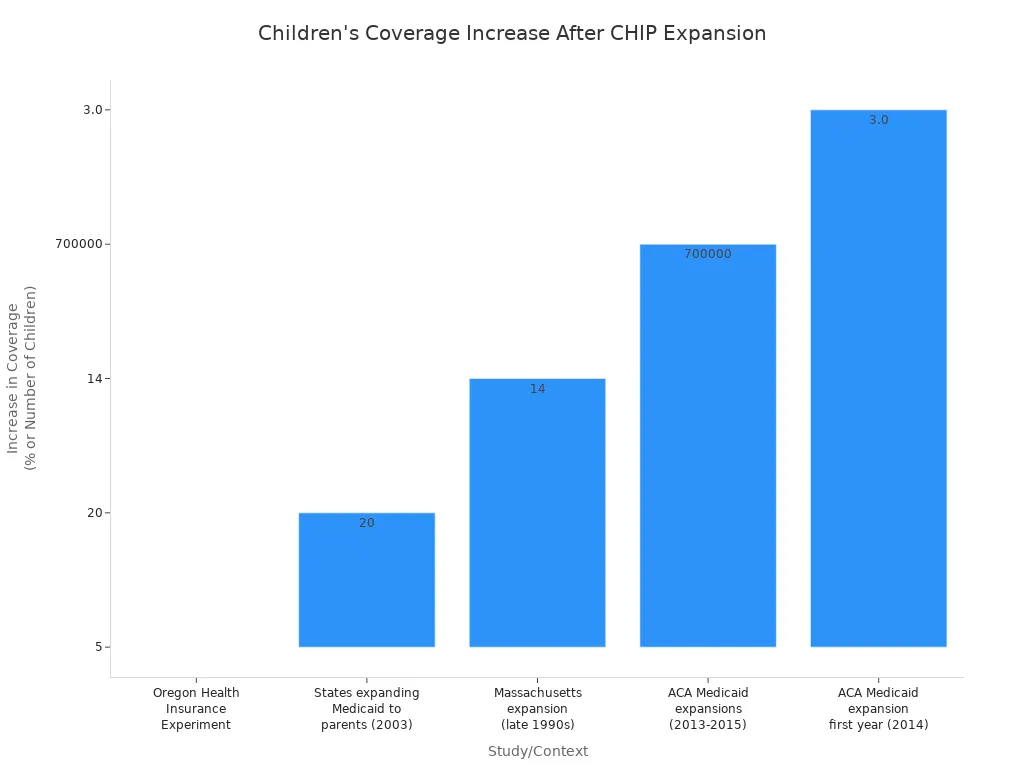
Research shows that when states expanded Medicaid or CHIP, more children got health insurance. For example, in Oregon, when adults gained Medicaid, children in those families were also more likely to get coverage. In Massachusetts, expanding Medicaid for adults led to a 14 percentage point increase in children’s coverage.
| Study/Context | Evidence of Increase in Children's Coverage |
|---|---|
| Oregon Health Insurance Experiment (Lottery) | 5% increase in children's coverage in households where adults gained Medicaid |
| States expanding Medicaid to parents (2003) | 20 percentage points higher Medicaid participation rate among children |
| Massachusetts adult Medicaid expansion | 14 percentage point increase in children's Medicaid coverage |
| ACA Medicaid expansions (2013-2015) | Over 700,000 children gained coverage |
| ACA Medicaid expansion first year (2014) | 3.0 percentage point increase in Medicaid/CHIP participation in expansion states |
State Flexibility and Program Design
States have a lot of freedom in how they run CHIP. They can decide who qualifies, what benefits to offer, and how to deliver care. States use different models, such as managed care, to make sure children get coordinated services. Some states place CHIP under their insurance department to reduce stigma and encourage more families to sign up.
State flexibility allows for:
- Setting their own income limits and eligibility rules within federal guidelines.
- Offering extra benefits like dental, vision, and mental health care.
- Using managed care to coordinate services and improve quality.
- Trying new ways to reach families, such as working with schools and community groups.
- Adjusting premiums and co-pays to help families transition to private insurance when possible.
A table below shows some state-level innovations that have improved coverage and outcomes:
| Innovation Category | Description and Impact |
|---|---|
| Administrative Placement | CHIP placed under insurance department to reduce stigma and boost enrollment. |
| Eligibility Expansion | Covered more children by raising income limits and including older children. |
| Comprehensive Benefits | Added preventive, dental, vision, hearing, and mental health services. |
| Managed Care Model | Used HMOs to provide coordinated care and provider choice. |
| Cost-sharing Mechanisms | Set affordable premiums and co-pays to help families and support program stability. |
| Outreach and Marketing | Partnered with community groups and schools to find and enroll eligible children. |
| Coordination with Medicaid | Made it easier for children to move between Medicaid and CHIP without losing coverage. |
| Evaluation and Quality Focus | Used outside experts to measure quality and focus on preventive care. |
States also use waivers to test new ideas and respond to local needs. This flexibility helps CHIP adapt to changing times and ensures that children in every state can get the care they need.
CHIP's Transformative Effects on Children's Health

Reducing Uninsured Rates
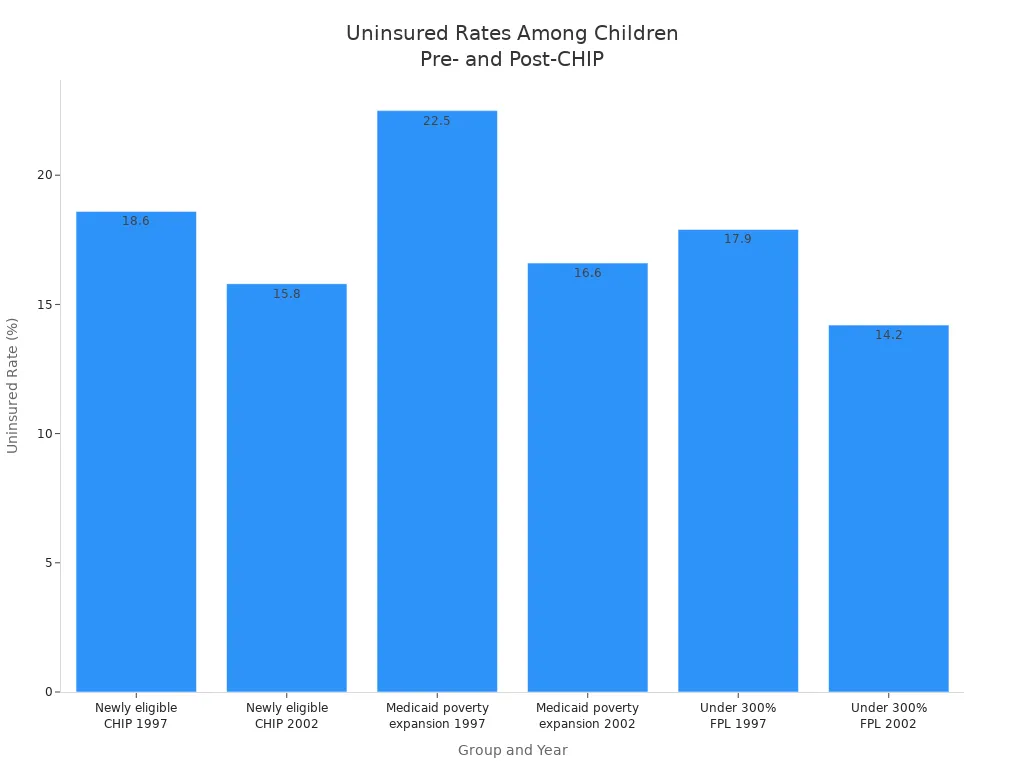
CHIP has played a major role in lowering the number of uninsured children in the United States. Before CHIP began, many children from working families could not get health insurance. Public coverage through Medicaid and CHIP increased sharply after the program started. The uninsured rate among children who became eligible for CHIP dropped from 18.6% in 1997 to 15.8% in 2002. Children eligible for Medicaid under poverty expansions saw their uninsured rate fall from 22.5% to 16.6%. Children in families earning less than 300% of the federal poverty level also saw improvements.
| Group | Year | Medicaid/CHIP Coverage (%) | Employer-Sponsored Insurance (%) | Uninsured Rate (%) |
|---|---|---|---|---|
| Newly eligible for CHIP | 1997 (pre-CHIP) | 7.1 | 70.3 | 18.6 |
| Newly eligible for CHIP | 2002 (post-CHIP) | 26.5 | 53.9 | 15.8 |
| Eligible for Medicaid under poverty expansions | 1997 (pre-CHIP) | 32.7 | 41.4 | 22.5 |
| Eligible for Medicaid under poverty expansions | 2002 (post-CHIP) | 48.4 | 32.6 | 16.6 |
| Children under 300% FPL | 1997 (pre-CHIP) | 28.3 | 50.6 | 17.9 |
| Children under 300% FPL | 2002 (post-CHIP) | 40.4 | 43.0 | 14.2 |
States with more robust CHIP programs have seen even greater progress. In 2021, expansion states had an uninsured rate of only 4.0% for children, while nonexpansion states had a rate of 7.1%. Expansion states also increased Medicaid and CHIP coverage by 1.6 percentage points, covering about 691,000 more children. Nonexpansion states relied more on Marketplace coverage, but their uninsured rates remained higher.
| State Type | Uninsured Rate in 2021 | Change in Uninsured Rate (2020-2021) | Change in Medicaid/CHIP Coverage (2020-2021) | Additional Coverage Notes |
|---|---|---|---|---|
| Expansion States | 4.0% | No change | +1.6 percentage points (35.5% total coverage) | Medicaid/CHIP coverage increased by ~691,000 children |
| Nonexpansion States | 7.1% | -1.6 percentage points | No change | Increase in Marketplace coverage by 1.2 percentage points |
CHIP has helped close coverage gaps for children in low-income families, especially in states that expanded eligibility and simplified enrollment.
Innovations in Enrollment and Outreach
CHIP has used creative strategies to reach more eligible children. Many families do not know their children qualify for coverage, so outreach and enrollment efforts are key. CHIP works closely with the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) to find uninsured children. WIC staff receive training to identify and refer families to CHIP and Medicaid. Some clinics have CHIP eligibility workers on site, making it easier for families to sign up.
- WIC staff learn about CHIP and Medicaid to help families.
- CHIP and Medicaid teams work with other child-serving programs to share resources and avoid repeating efforts.
- Some clinics let WIC staff check if children are likely eligible for CHIP or Medicaid.
- Families see posters and get brochures about CHIP in WIC clinics.
- WIC hotlines and joint applications include CHIP information.
CHIP also uses mail-based outreach, posters, and brochures to reach families. Messages that highlight dental benefits often get more attention. Outreach works best when combined with other public programs, such as SNAP. Over half of families who responded to SNAP outreach also applied for Medicaid. These efforts show that CHIP can reach hard-to-reach groups, but challenges remain. Some families face language barriers, low health insurance literacy, or fear due to immigration status. States that remove premiums and make enrollment easier see higher participation.
Note: About 40% of children enrolled in Medicaid or CHIP still face at least one barrier to care, such as trouble getting preventive visits or delays in needed services. Adolescents, Black children, and those in single-parent households are at higher risk for these barriers.
Improving Health Outcomes
Children with CHIP coverage experience better health than those without insurance. More children receive preventive care, such as checkups, vaccines, and dental visits. Medicaid and CHIP expansions have helped about 6 million children get preventive services. Infant and child mortality rates have dropped, and preventable hospitalizations have decreased. CHIP also supports long-term success by improving school attendance, graduation rates, and even future earnings.
| Health Outcome Category | Improvement Attributed to CHIP Participation and Medicaid Expansions |
|---|---|
| Access to Preventive Care | About 6 million children began receiving preventive care due to Medicaid and CHIP expansions. |
| Infant and Child Mortality | Declines in infant and child mortality rates following expansions of public health insurance. |
| Preventable Hospitalizations | Reductions in preventable hospitalizations among children after Medicaid and CHIP expansions. |
| Long-term Health and Socioeconomic Outcomes | Beneficiaries have higher educational attainment, increased earnings, better self-reported health, and lower mortality and hospitalization rates compared to non-beneficiaries. |
| Birth Outcomes | New mothers covered by Medicaid as infants are giving birth to healthier children today, showing intergenerational health benefits. |
Children with CHIP coverage have similar or better rates of preventive care compared to those with private insurance, and their families pay less out of pocket. Uninsured children have the poorest access to care and the highest unmet needs. CHIP also narrows health gaps for Black, Brown, and Indigenous children. The Affordable Care Act made it easier to enroll in CHIP and Medicaid, which helped reduce racial and ethnic disparities in coverage. States that expanded Medicaid saw bigger drops in infant mortality, especially among Black infants.
- CHIP provides affordable, comprehensive coverage for children in working families.
- It ensures access to preventive care, dental and vision services, and mental health support.
- The program helps families avoid financial hardship and supports children's academic success.
CHIP has transformed children's health by making care more accessible, reducing health disparities, and improving outcomes for millions of children.
CHIP has redefined children’s health coverage by expanding access and improving outcomes. Funding instability and gaps in reaching eligible children remain. Policymakers recommend longer continuous eligibility, streamlined enrollment, and stable funding. New federal rules and state innovations promise better coverage, but ongoing support is essential for future progress.
FAQ
What is CHIP?
CHIP stands for the Children’s Health Insurance Program. It helps children in families who earn too much for Medicaid but cannot afford private insurance.
Tip: CHIP covers doctor visits, dental care, and more.
Who can get CHIP coverage?
Children under 19 in families with incomes below a certain level can qualify. Some states also cover pregnant women and lawfully present immigrants.
- Each state sets its own rules.
- Families can check eligibility online.
How does CHIP help children stay healthy?
CHIP pays for checkups, vaccines, dental visits, and mental health care. Children with CHIP see doctors more often and miss fewer school days.
| Service | Covered by CHIP? |
|---|---|
| Checkups | ✅ |
| Vaccines | ✅ |
| Dental Care | ✅ |
| Mental Health | ✅ |